Skip to content
Alkali Injury
Alkaline compounds cause saponification of the fatty acids in cell membranes, which penetrates the ocular surface epithelium as well as deeper cellular structures.
Corneal and conjunctival epithelium, goblet cells, stromal keratocytes, corneal extracellular matrix, blood vessels, ciliary body and trabecular meshwork may be damaged.
Clinical Features
Immediate rise in the pH following alkaline solution exposure to eye.
Symptoms: ocular pain, lacrimation, blepharospasm.
Signs:
In mild cases: epithelial erosion, mild corneal haze and conjunctival injection.
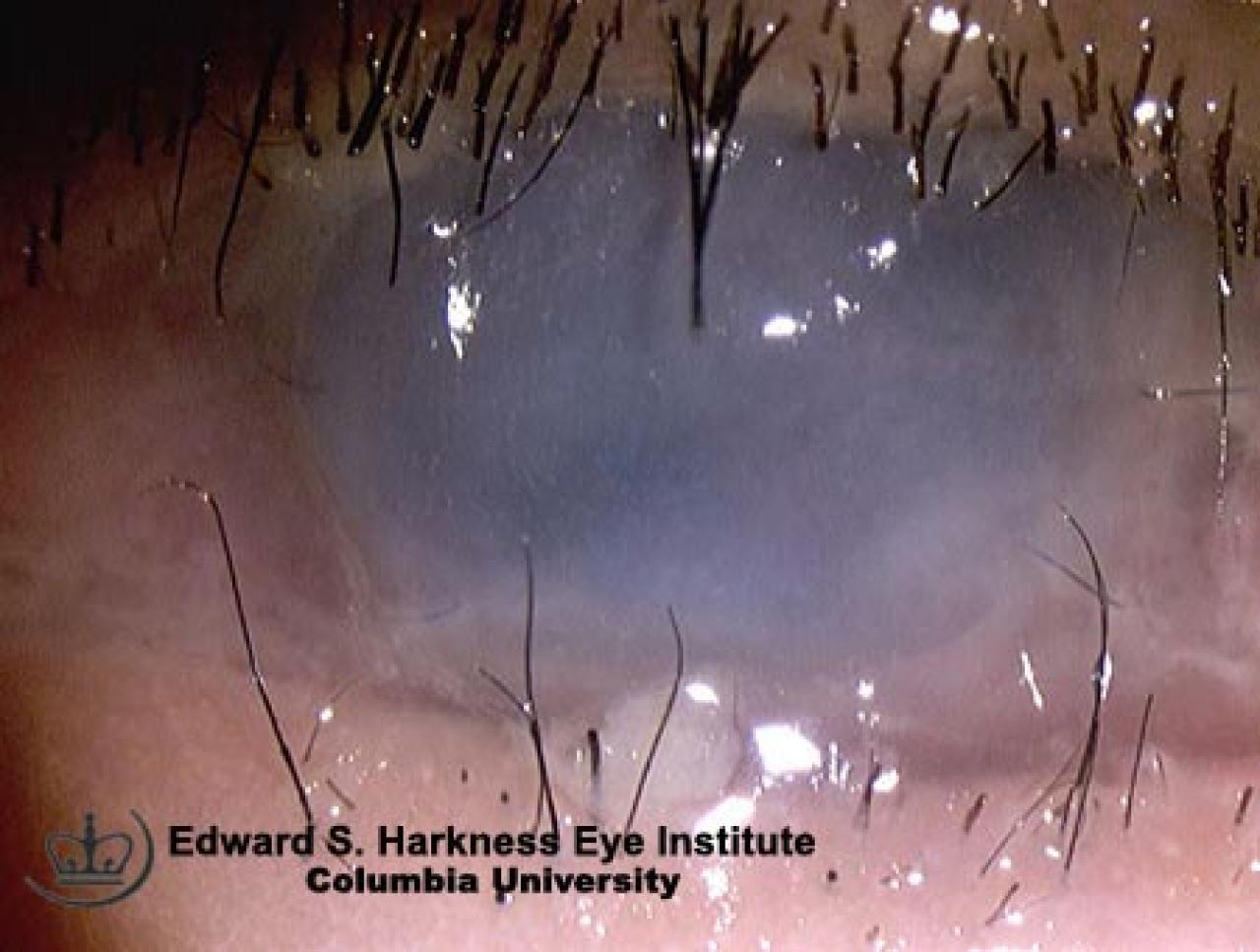
In moderate cases: cornea may opacify with slight ischemia of limbus.
In severe cases: significant ischemia of the sclera, avascularity of the limbus, blanching of conjunctiva and severe corneal haze.
Complications
Eyelid scarring
Corneal opacification, severe dry eye, corneal ulcer, perforation with potential secondary intraocular infection
Conjunctival scarring, symblepharon or ankyloblepharon
Aqueous dynamic changes with increased or decreased intraocular pressure
Cataract and phthisis bulbi
Management
Immediate irrigation of eye until the pH of the cul-de-sac has returned to neutrality. (pH= 7.0)
Remove foreign bodies and sweep fornices.
Cycloplegic drops.
Topical prophylactic broad-spectrum antibiotics.
Analgesic.
Topical steroid for I week to decrease the inflammatory response.
Control of intraocular pressure.
Insertion of methymethacrylate ring into cul-de-sac might prevent symblepharon and conjunctival fibrosis.
Consider doxycycline for its collagenase inhibitor effect.
Vitamin C 2 gram qid to promote collagen synthesis.
During re-epithelialization phase:
Intense lubrication with preservative free tear is essential
Soft contact lens maybe helpful
Patching or temporary tarsorraphy
Surgical treatment:
Limbal stem cell transplantation with or without amnioniotic membrane
Conjunctival graft
Corneal transplantation
Back to top