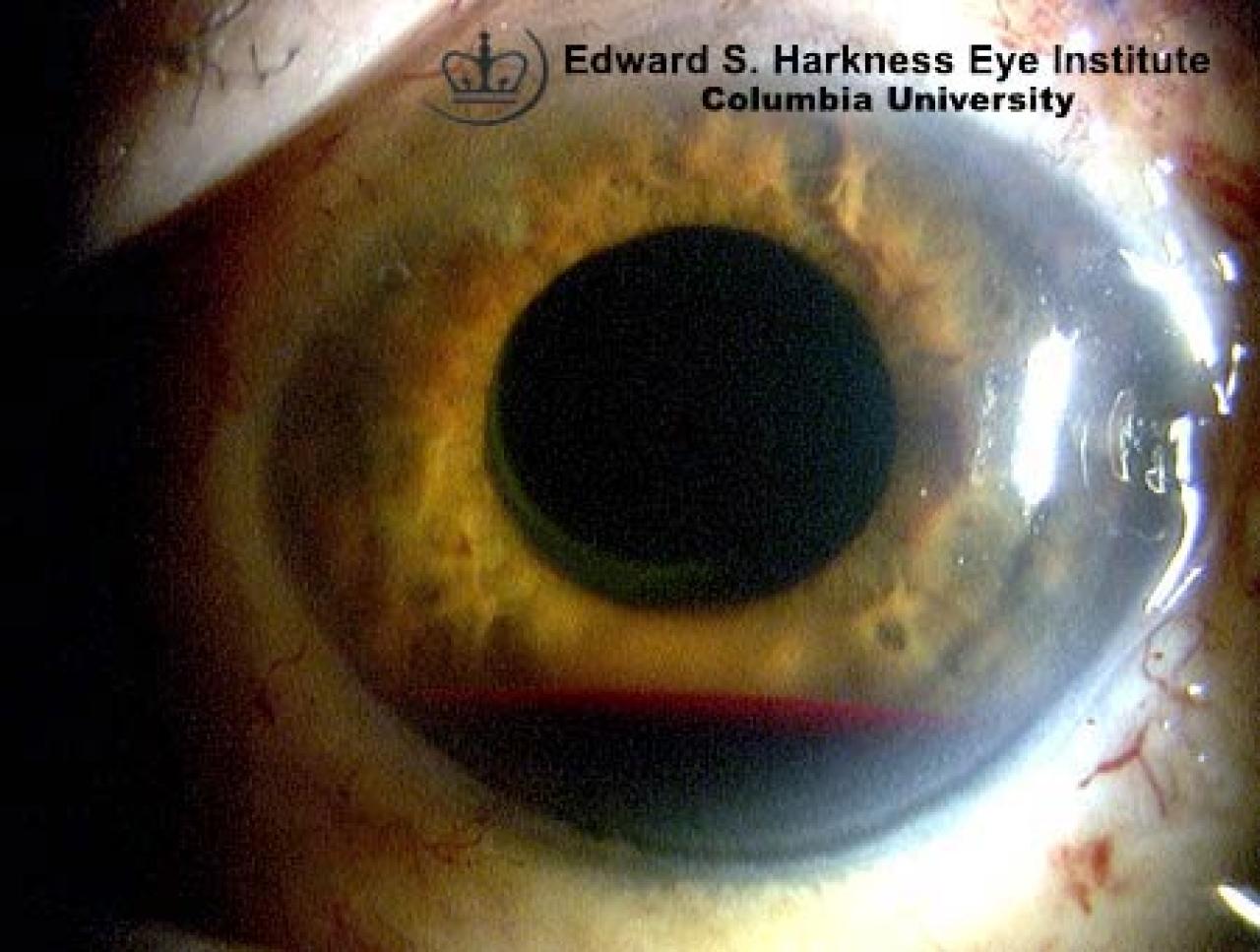
Accumulation of blood within the anterior chamber.
Frequently is the result of blunt eye trauma.
The source of bleeding is usually a tear in the anterior face of the ciliary body.
Clinical Features
Intraocular pressure elevation following eye injury as a result of mechanical obstruction of the trabecular meshwork by the clotted blood
Rarely, pupillary block from severe hyphema may occur, causing acute glaucoma.
Complications
Prolonged unresolved hyphema
Persistent elevation of intraocular pressure complicated with optic nerve damage
Corneal blood staining and corneal endothelial decompensation.
Management
Usually supportive after ruling out other possible coexisting medical problems such as coagulopathy or Sickle cell anemia.
Small hyphemas generally resolve in 4 to 5 days.
Systemic antifibrinolytic agents such as aminocaproic acid is reported to prevent secondary bleeding.
Topical or systemic glaucoma agents.
Surgical treatment to wash out the blood in cases with intractable intraocular pressure elevation, unresolved total hyphema, corneal blood staining and sickle cell patient.