Proliferative Diabetic Retinopathy (PDR)
- Characterized by growth of new vessels on the surface of the retina.
Clinical Features
- Symptoms: progressive loss of vision, particularly in those who are not properly followed or treated.
- Signs:
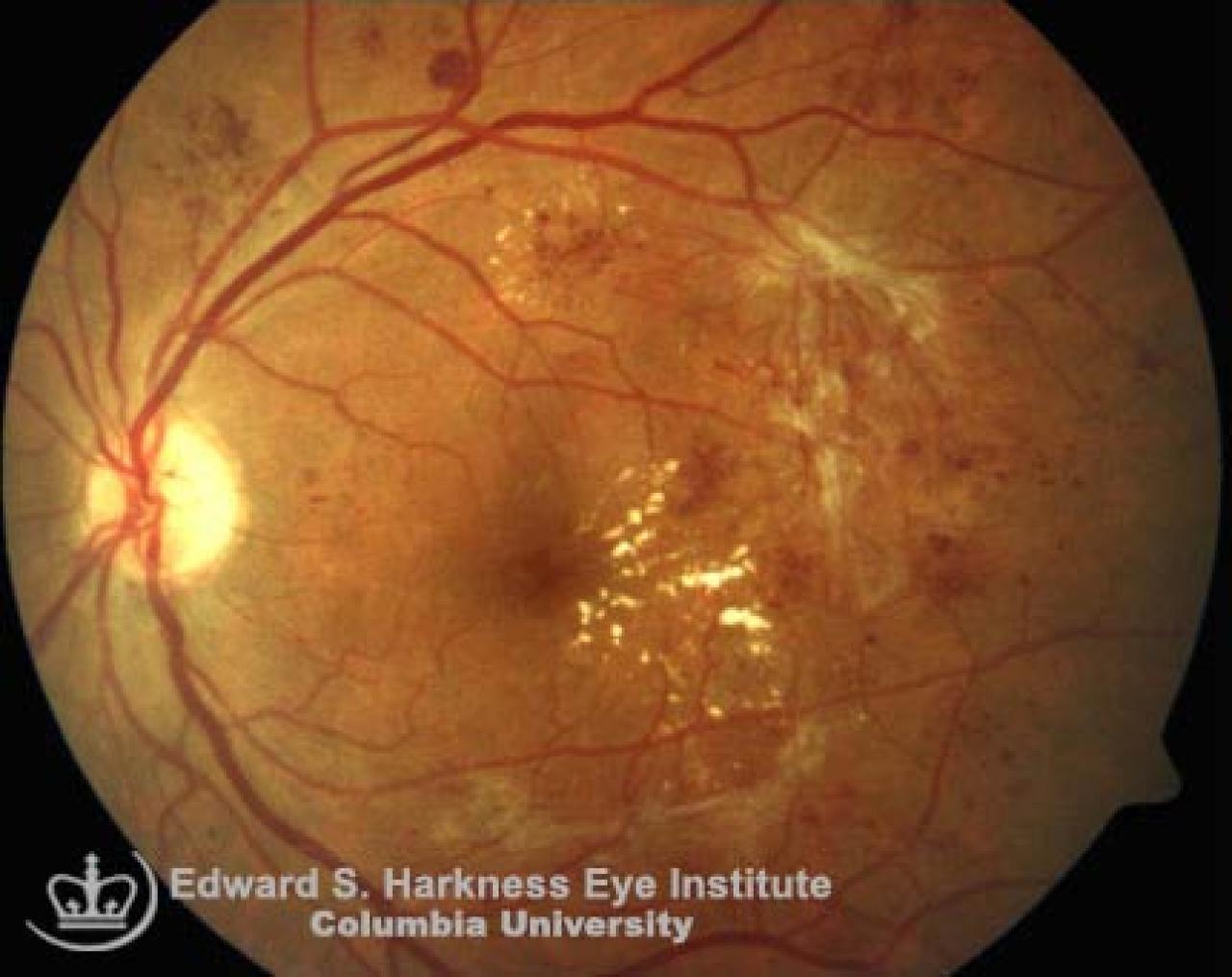
- Fine to severe loops of new vessels that may grow on the optic disc: neovascularization of the disc (NVD) or elsewhere (NVE)
- In the anterior segment, PDR is manifested by neovascularization of the iris (NVI), the angle (NVA) and may eventually complicated with neovascular glaucoma
- These new vessels may leak and resulting in retinal edema. They are also fragile and prone to bleed
- Opaque fibrovascular proliferation tissue often appears on the internal limiting membrane (adjacent to the new vessels) and becomes adherent to the vitreous
- Contraction of this fibrovascular tissue may lead to:
- Distortion or dragging of the macula
- Mild to extensive retinal detachment
- Avulsion of retinal vessels and vitreous hemorrhages
Risk Factors
- Duration of the diabetes
- 30-34 years of diabetes increase the risk of retinopathy by 65%
- Overt albuminuria
- High level of blood total cholesterol and LDL
- Others: race, cigarette smoking, alcohol
Management
- Strict blood glucose, blood pressure and cholesterol control.
- Photocoagulation for clinically significant macular edema prior to scatter (panretinal) photocoagulation (PRP).
- Consider PRP in severe proliferative diabetic retinopathy.
- Consider additional PRP if incomplete regression is observed, increasing of the extent of vitreous hemorrhage or worsening of overall vitreoretinal condition.
- Vitrectomy.
- Experimental treatments; Depo steroid injection for diabetic macular edema, systemic protein kinase-C inhibitor and aldolase reductase inhibitor.